Is Anger Issues Genetic: What Heredity Can Mean for IED
If you’ve been asking, is anger issues genetic, you’re not alone. Anger can feel automatic—especially when intense outbursts seem to “run in the family.” But genes are only part of the story. Your upbringing, stress load, and learned coping habits can shape how anger shows up and how quickly it escalates. This article explains what research suggests about genetics and environment, with a specific look at Intermittent Explosive Disorder (IED). It’s for education and self-understanding only, not a diagnosis or medical advice. If you want a structured way to reflect on your reactions, you can explore a private IED assessment tool.
The Short Answer: Is Anger Genetic, Environmental, or Both?
The nature vs. nurture debate is rarely black and white. If you’re asking, is anger issues genetic or environmental, the most accurate answer is usually both.
A helpful frame is: biology may influence sensitivity and impulse control, while environment influences triggers, habits, and recovery.
How Genetics and Environment Interact
Some people may inherit traits linked to a stronger stress response or faster emotional escalation. But whether that vulnerability turns into frequent explosive reactions depends a lot on life experience.
- Genetic predisposition can shape reactivity and self-control.
- Environmental factors like family conflict, trauma, chronic stress, and poor sleep can intensify reactions over time.
You can inherit a tendency, not a guarantee.
Why One Sibling Struggles More Than Another
Even in the same family, siblings don’t share identical biology or identical experiences. One person may be more sensitive to stress, while another has stronger impulse control or different protective experiences. This is one reason anger can seem hereditary, but still vary widely from person to person.
The Biology of Anger: What Science Says About Your Genes
To understand is anger genetic, it helps to look at the brain systems involved in threat detection and regulation. There isn’t one single “anger gene.” Instead, many factors can influence how quickly anger rises and how hard it is to pause.
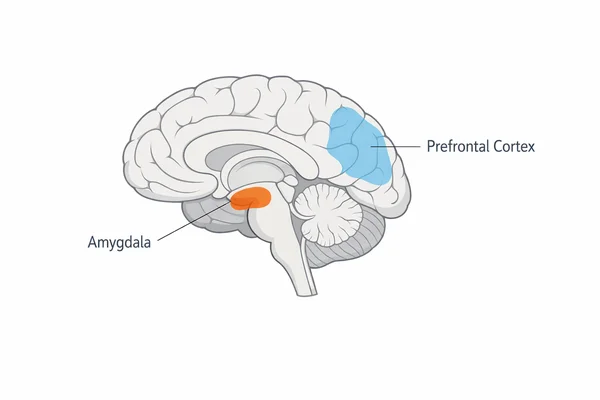
The Amygdala and the Fight-or-Flight Response
The amygdala helps detect threat and trigger fight-or-flight. When it’s highly reactive, everyday situations can feel urgent. The prefrontal cortex supports planning and inhibition. When regulation is weaker, anger can surge before you have time to think.
Serotonin and Impulse Control
Serotonin is linked to mood regulation and impulse control. Differences in how the brain produces, uses, or clears serotonin may affect how easy it feels to slow down and choose a different response. Genetics may influence these systems, but they don’t dictate outcomes on their own.
Is Intermittent Explosive Disorder Hereditary?
Everyone gets angry sometimes. IED is different: it involves repeated, impulsive outbursts that feel out of proportion to what’s happening. Evidence suggests IED can cluster in families, which is why people ask is anger issues hereditary in the first place.
When Anger Becomes a Disorder Pattern
IED is generally described by:
- recurrent outbursts that reflect difficulty controlling aggressive impulses
- reactions that are out of proportion to the trigger
- episodes that are impulsive rather than planned, and not done to gain something tangible
Only a qualified professional can diagnose IED, and they look at patterns over time—not a single incident.
What Family Patterns Can and Can’t Tell You
Family history may increase risk, but it doesn’t determine your future. Shared genetics can matter, and so can shared environment (how conflict was handled, what stressors were present, and what coping skills were modeled). The same family background can lead to different outcomes depending on support, skills, and context.
Understanding Your Patterns: Self-Assessment vs. Diagnosis
If these descriptions feel familiar, it can help to separate reflection from diagnosis. You can learn a lot from noticing your own patterns without labeling yourself.
Why a DNA Test Can’t Diagnose Anger
There is no clinical DNA test that can confirm anger issues or IED. A clinician evaluates behavior patterns, impact on relationships/work/safety, and what else might be contributing.
A Gentle Next Step: A Private Self-Check
Because patterns matter, a structured self-check can be useful. It can help you notice triggers, speed of escalation, and what happens after an outburst. If you’d like a starting point, you can try a confidential Intermittent Explosive Disorder self-check to organize what you’re experiencing and decide what support might help.
Nature vs. Nurture: Are Anger Issues Genetic or Learned?
People often ask are anger issues genetic or learned. For many, it’s both—just in different proportions.
The Impact of Modeling and Family Habits
Children learn how to handle frustration by watching adults. If yelling, threats, or intimidation were common ways to cope, those reactions can become “normal,” even if you disliked them. Over time, learned habits can look like personality traits.
Trauma, Chronic Stress, and Emotional Regulation
Trauma and chronic stress can keep the nervous system on high alert. When your body is constantly bracing for danger, anger can become a fast defense. This doesn’t mean your past “caused everything,” but it can explain why certain triggers hit so hard.
Signs Your Anger Might Be More Than a Bad Temper
These signs can help you tell the difference between ordinary frustration and a more serious pattern.
1. Your Reaction Is Disproportionate to the Trigger
A small mistake leads to a major surge of anger that doesn’t match the situation.
2. The Anger Has a Rapid Onset
It feels like a switch flips. You go from calm to overwhelmed quickly, and it’s hard to slow down once it starts.
3. You Feel Remorse or Exhaustion Afterward
After the episode, you may feel shame, confusion, or deep fatigue, and regret what you said or did.
Can You Manage Genetic Anger Issues?
Some people wonder is anger management genetic, as if change depends on DNA. Genetics may influence your starting point, but skills and support can change what happens next.
Rewiring Habits With Skills and Support
Approaches like Cognitive Behavioral Therapy (CBT) often focus on practical steps:
- identify early body signals (heat, tight chest, jaw tension)
- challenge threat-based thoughts before they escalate
- practice alternative responses until they become more automatic
Some people also discuss medication options with a clinician, especially when mood, impulse control, or co-occurring concerns are involved. Any treatment choice should be personalized and guided by a professional.
A Simple If-Then Plan
- If my anger spikes fast, then I name it: This is anger, not danger.
- If I feel close to exploding, then I create distance for two minutes.
- If I’m calmer, then I return and speak in one clear sentence.
Closing Thoughts: Taking Back Control
So, is anger issues genetic? Genetics can play a role, especially in IED-like patterns. But your environment, coping skills, and support system also matter—and change is possible. Understanding the “why” behind your reactions isn’t an excuse; it’s a starting point for better choices.
If you want a structured snapshot of your patterns to discuss with a professional, you can explore the free IED screening questionnaire.
Frequently Asked Questions
Is there a genetic test for anger issues?
No. There isn’t a clinical genetic test that diagnoses anger issues or IED. Evaluation is based on patterns over time, context, and impact, usually assessed by a qualified professional.
Are anger issues a sign of mental illness like ADHD?
Anger can overlap with conditions involving impulse control or emotional regulation, including ADHD. But anger alone doesn’t confirm any diagnosis, and different causes can look similar.
Do tempers run in families?
Sometimes. Temper and explosive anger patterns can cluster in families due to a mix of shared genetics and shared environment, including learned coping habits and stress exposure.
Can you unlearn anger if you grew up in an angry household?
Often, yes. Many people learn healthier coping skills through therapy, practice, and supportive relationships, even if anger was normalized in childhood.
Is aggression a learned behavior or a biological trait?
It can be both. Biology may influence reactivity, while learning and experience shape how aggression is expressed and how effectively it can be managed over time.